From Public Health Watch:
HEMPHILL, Texas — Sarah Gipson knew something was wrong when the normally chatty sonogram technician fell silent and called for the doctor.
Gipson was in the 32nd week of her high-risk pregnancy, and she felt horrible. She was seeing stars, had constant ringing in her ears, and had been on bed rest for several weeks.
Still, she wasn’t alarmed.
“It wasn’t anything abnormal for me to feel terrible,” she said.
That Halloween Day in 2024, however, was different. The doctor told her she’d lost all amniotic fluid — that the baby was “dry” and had to be delivered immediately, both for the baby’s sake and for her own.
But Gipson, who was expecting her first child, was all alone at the doctor’s office in Nacogdoches that day; she’d made the hour-long drive by herself from her home in Hemphill in Sabine County. Her mother arrived just in time for the surgery.
“My child could have died,” Gipson said. ”I could have died. Other people could have lost their children in childbirth. Something could happen on the way, because they’re flying 90-to-nothing trying to get there. … Human life, the loss of a human life, is one of those things that you should care about.”
Gipson is one of thousands of women across Texas living in a maternal healthcare “desert,” with limited access to care during pregnancy, according to an analysis by Public Health Watch of data published in a May 2024 report by the Texas Organization of Rural and Community Hospitals (TORCH).
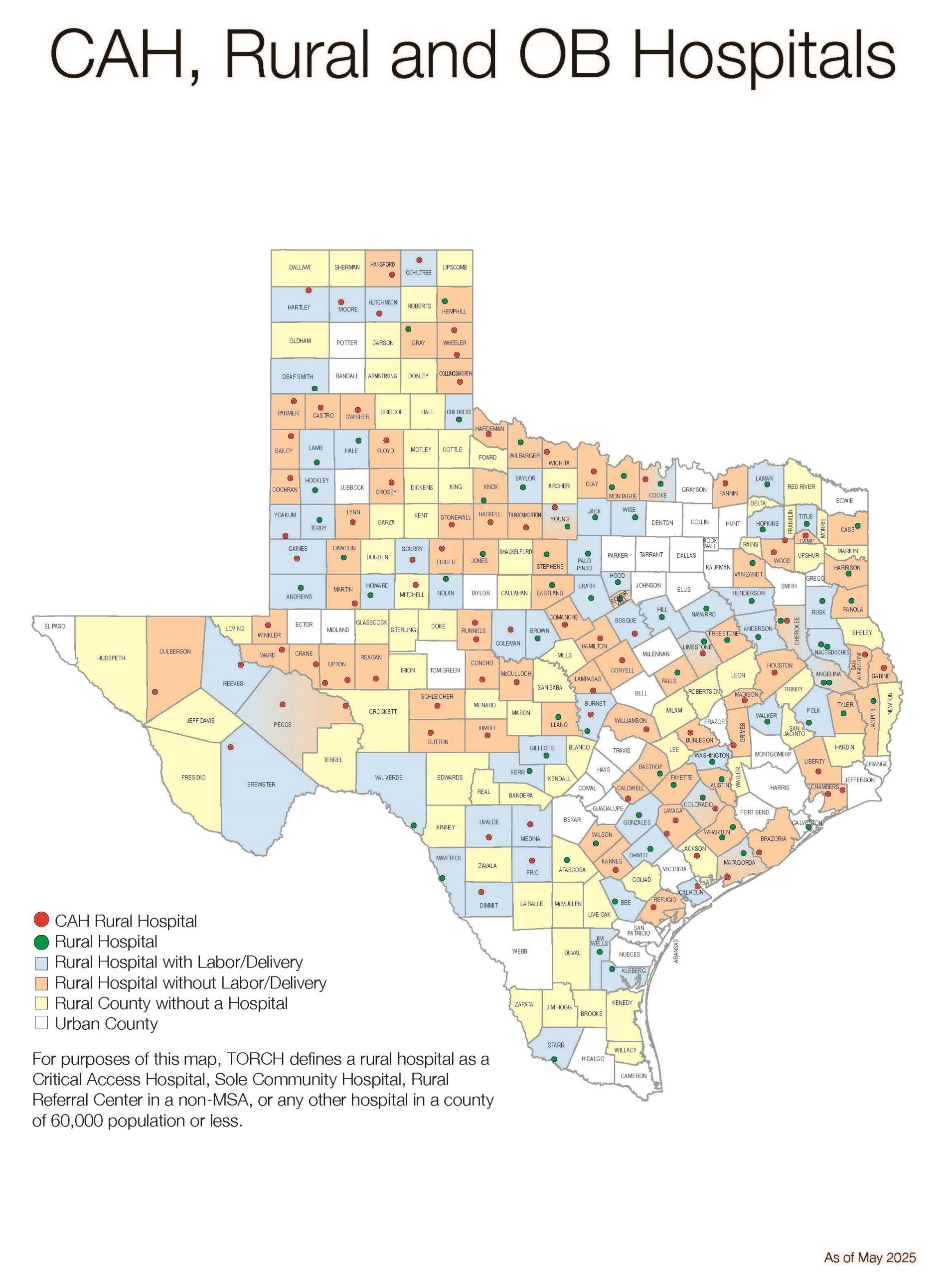
The Texas Organization of Rural and Community Hospitals (TORCH) gathered county-by-county data from across Texas on the availability of hospitals and labor-and-delivery units in rural counties. The analysis was released in a May 2024 report. Credit: Courtesy of Texas Organization of Rural and Community Hospitals
Of the more than 200 rural counties in Texas, about 70 percent have no hospital at all or have hospitals that don’t have facilities for delivering babies.
Maternal access is even worse in East Texas, where more than 80 percent of the nearly 60 counties stretching from Oklahoma to the Gulf Coast are considered rural. More than 72 percent of those counties lack hospitals or labor-and-delivery units.
The cash-strapped rural hospitals can’t make enough money from private insurance or Medicaid to cover the costs of providing maternal care, according to John Henderson, TORCH chief executive officer.
“The pure economics of it are just problematic,” he said.
In the last five years, more than 100 rural hospitals nationwide have stopped delivering babies, leaving fewer than half of rural hospitals across the country with labor-and-delivery services, according to a report from the Center for Healthcare Quality and Payment Reform released in January.
Others are at risk of closing their doors altogether. About one-third of the 2,256 rural hospitals across the United States are at risk of closure, with nearly half of those at immediate risk, according to the report.
In Texas, more than half of rural hospitals are at risk of closure, with about 15 percent at immediate risk. About 20 percent of the state’s labor-and-delivery units are also facing possible closure.
The result is that rural Texas women often face financial and emotional stress — and sometimes dangerous complications during pregnancy — that they might have avoided if they’d had better access to maternal healthcare, according to more than a dozen women, healthcare workers, advocates and industry officials who spoke to Public Health Watch about their experiences.
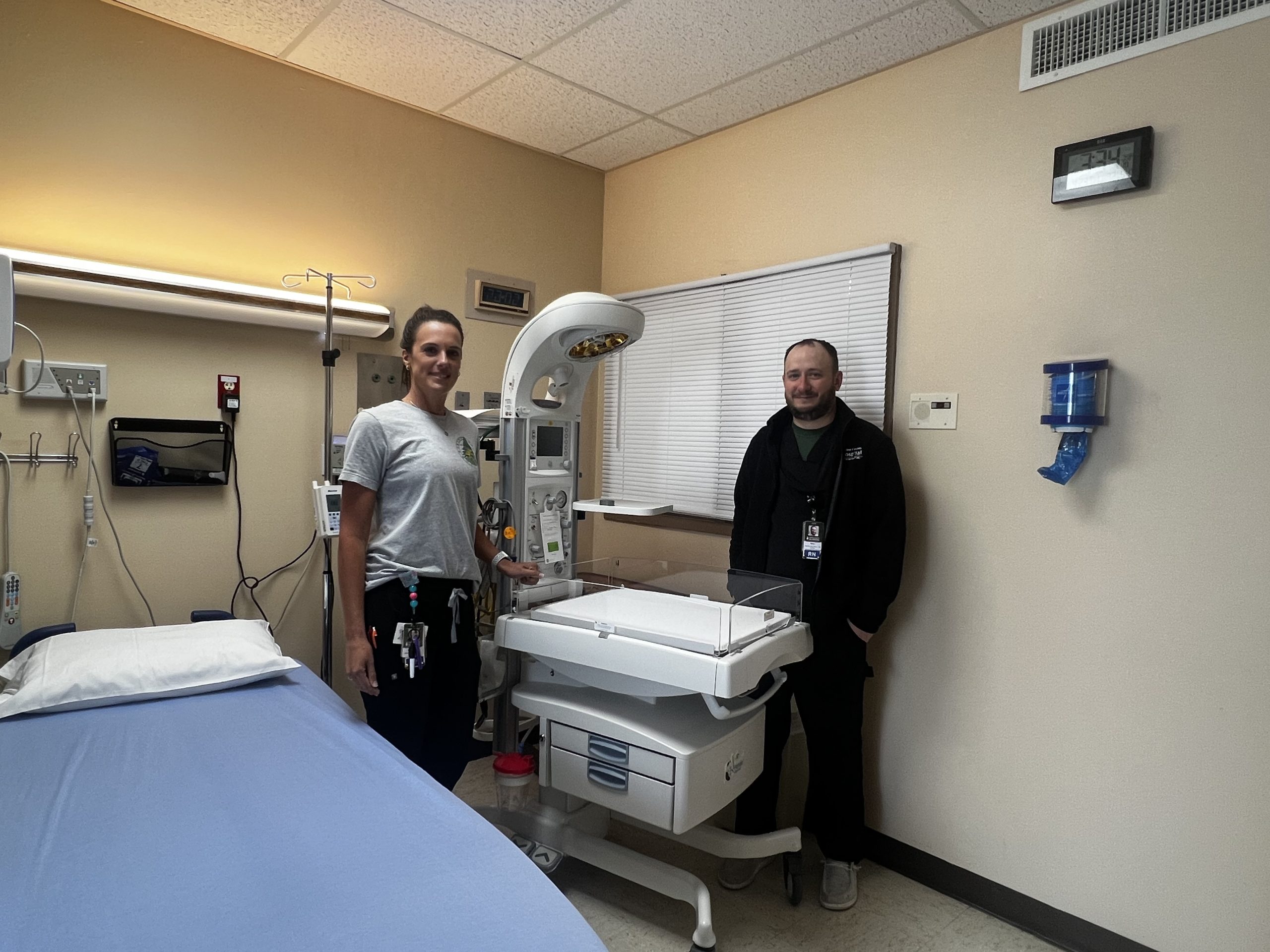
Sabine County is among the counties without a labor-and-delivery unit, though discussions are underway to expand services at Sabine County Hospital in Hemphill, which closed its delivery unit in 2000.
A new physician is stepping in as a family medicine doctor with special training and will work with hospital administrator Kaylee McDaniel to find ways to better serve women in the community, perhaps initially by offering access to check-ups and monitoring.
“Rural Texans matter, too,” McDaniel said.
Road warriors
An enormous surgical light still hangs from the ceiling of what used to be the labor-and-delivery room at Sabine County Hospital, an enduring reminder of state-of-the-art services that women in the county once received.
The room is now used for storage, with just one rack of obstetrics supplies pushed against a wall amid a collection of other shelves and boxes. The medical equipment is too old to be used for deliveries.